Overview/Terminology

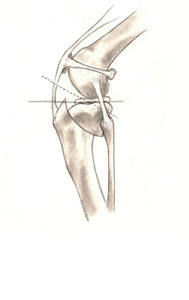
The cranial cruciate ligament (or CCL, see Figure 1) is one of the most important stabilizers inside the knee (also called “stifle”) joint, the middle joint in the back leg. In humans the CCL is called the anterior cruciate ligament (ACL). The meniscus (see Figure 1) is a cartilage-like structure that sits in between the shin and thigh bone. It serves many important functions in the joint such as shock absorption, proprioception, and load bearing, and is frequently damaged when the CCL is injured. Rupture of the CCL is one of the most common reasons for hind limb lameness, pain, and subsequent arthritis.
The development of this problem in dogs is much more complex than in humans. Furthermore, dogs suffer from different degrees of rupture (partial, complete). Hence, the condition is frequently referred to as “cranial cruciate disease” (CCLD) rather than “cranial cruciate ligament rupture” (CCLR). While the degree of lameness with CCLD varies, it invariably causes arthritis in the long term. For athletic patients, surgery in combination with joint supplements is recommended to slow down progression of arthritis and to eliminate/minimize lameness, though many non-surgical treatment options are also available.
Causes
In humans, trauma (such as skiing, football, or soccer injuries) is the most common reason for injury of the ACL. This “traumatic” rupture can happen in dogs but is quite rare. Most commonly, CCLD is caused by a combination of many factors, including aging of the ligament (degeneration), obesity, poor physical condition, conformation, and breed. In other words, the ligament injury is a result of subtle, slow degeneration that has been taking place over a few months, or even years, rather than the result of sudden trauma to an otherwise healthy ligament. This difference between people and dogs explains two important features of canine CCLD:
- At least half of the dogs that have a cruciate ligament problem in one knee will likely, at some future time, develop a similar problem in the other knee.
- Partial tearing of the CCL is common in dogs and frequently progresses to a full tear over time.
Incidence and Prevalence
Cruciate disease affects dogs of all sizes and ages and rarely cats. Certain dog breeds are known to have a higher incidence of CCLD (such as Rottweiler, Newfoundland, Staffordshire Terrier, Mastiff, Akita, Saint Bernard, Chesapeake Bay Retriever and Labrador Retriever), while others are less often affected (such as Greyhound, Dachshund, Basset Hound, and Old English Sheepdog). It has been shown that female and neutered dogs are at greater risk of developing CCLD. However, the exact reason for this finding is unknown and the benefits of neutering may outweigh this increased risk. Recently, a genetic mode of inheritance has been shown for Newfoundlands.
Signs and Symptoms
As previously mentioned, progressive degeneration of the CCL from very mild partial tearing to a complete tear in the later stages of the disease is common in dogs. Because of this progression, you may not notice a severe lameness initially, especially if both knees are affected. One common symptom is that dogs will not sit “square” anymore but rather put their leg(s) out to the side when they sit down. You may also observe that your dog has difficulty rising, trouble jumping into the car, as well as a decreased activity level. Muscle atrophy (decreased muscle mass in the affected leg), decreased range of motion, a popping noise (which may indicate a meniscal tear), and swelling on the inside of the shin bone (fibrosis or scar tissue) are other symptoms. Many dogs will shift their weight away from the damaged leg when they stand but the lameness is less obvious during walking especially with partial tears of the CCL. When a partially damaged ligament ruptures completely or the meniscus becomes damaged your dog may also become non-weight bearing lame and may hop on three legs. This change in lameness may happen suddenly, usually without major trauma (a minor traumatic event may cause the partially torn ligament to rupture completely). Dogs with chronic (late stages) of CCLD usually show symptoms associated with arthritis (decreased activity, stiffness, unwillingness to play, pain etc.).
Risk Factors
Poor physical condition and excessive body weight are risk factors for the development of CCLD. Both of these factors can be influenced by pet owners. To accomplish a good fitness level regular activity and avoiding intermittent excessive activity by usually inactive dogs (“weekend warrior syndrome”) is advised. Regular exercise will also help to avoid obesity.
When to Seek Veterinary Surgical Advice
It is advisable to contact your veterinarian if your dog shows an obvious lameness that persists for longer than a day or is in obvious pain. Frequently, a sudden lameness is due to a soft tissue injury and may resolve within a couple weeks. If the lameness is minor and no significant pain is associated with it, you may rest your animal (no off-leash activity) for a few days and see whether the lameness disappears. Please do not administer aspirin or other over the counter medications because those may be harmful to your pet. As a general rule, it is always better to have your animal evaluated by your veterinarian.
Exam, Screening Tests, and Imaging
Diagnosing complete tears of the CCL is easily accomplished by a combination of observation of your pet’s gait, palpation of the knee and radiographs (X-rays). For early partial tears, however, it can be a bit more complicated and may sometimes require advanced imaging such as MRI or surgical exploration to physically look at the ligament. X-rays are usually taken to confirm the presence of joint effusion (fluid accumulation in the joint which indicates that there is a problem within the joint), the degree of arthritis, to aid in surgical planning and to rule out concurrent disease conditions such as bone cancer. For certain treatments, like tibial plateau leveling osteotomy (TPLO) and tibial tuberosity advancement (TTA), specific X-rays are required and your surgeon may need to repeat radiographs of the knee even if your veterinarian has already taken some. Specific palpation techniques that veterinarians use to confirm a problem with the CCL are the “cranial drawer test” and the “tibial thrust test.” These tests confirm abnormal motion in the knee and hence a rupture of the CCL. X-rays do not show the status (i.e. intact or damaged) of the CCL or the meniscus because those structures cannot be seen on X-rays. Therefore, it is crucial that the surgeon evaluate both of these structures (meniscus and the cruciate ligament) when performing the chosen surgical repair. This can be done either via an arthrotomy (opening of the joint) or with the use of a minimally-invasive camera (arthroscope) and is generally combined with the surgical procedure itself because both procedures require full anesthesia and clipping of the animal.
Differential Diagnoses

While CCLD is one of the most common reasons for persistent hind limb lameness in dogs, there are numerous other causes for pain and lameness in the rear limbs of dogs. It is important to rule out other problems to determine the best treatment for your pet. Other conditions may include hip dysplasia, joint sprains or muscle strains, knee cap displacement (which may also occur in combination with CCLD), neurologic disease (such as a ruptured disc), bone or soft tissue cancer, fractures, joint dislocations (luxations), tendon rupture (Achilles tendon) and panosteitis (an inflammatory bone disease seen mainly in young, large breed dogs) or osteochondrosis (a cartilage disease).
Complications
The most common complication caused by CCLD is long-term impairment due to arthritis. Other complications associated with arthritis and CCLD include loss of range of motion in the joint, muscle atrophy, and loss of full function of the limb, as well as decreased activity. Unfortunately, neither human nor veterinary surgeons are able to completely restore normal joint anatomy and function. Even with surgery some progression of arthritis is expected. It is important to understand that arthritis is a non-reversible disease and hence everything should be done to prevent its development or progression. Therefore, two steps are crucial when treating CCLD:

- Surgical repair and
- Medical management of arthritis
The second most common complication caused by CCLD is tearing of the meniscus. Due to the instability in the knee joint, the inside (medial) meniscus frequently gets damaged. This can happen during the initial injury or even later after surgical repair of the CCL. Meniscal damage in dogs is addressed by removing the damaged parts of the meniscus because it is too small to repair. A meniscal tear is very painful and if a damaged meniscus is left in place the animal will not regain full function. Therefore, removal of the damaged parts of the meniscus (if present) will be performed by your surgeon when he or she performs the procedure chosen to address the knee instability. Lastly, as previously mentioned, rupture of the CCL in the opposite limb happens in more than 50% of the animals.
Treatment Options: Surgical Treatment
There are many treatment options for CCLD but the first major decision is between surgical treatment and non-surgical (also termed conservative or medical) treatment/management. The best option for your pet depends on many factors such as your pet’s activity level, size, age and conformation as well as the degree of knee instability.
In general, surgical treatment is recommended for CCLD because it is the only way to permanently control the instability in the stifle joint and to evaluate the structures within the joint. In other words, surgery addresses the two major problems seen with CCLD: stifle instability because of loss of the CCL and damage to the inside meniscus commonly seen in conjunction with CCLD. Again, meniscal problem will be addressed by your surgeon by removing the damaged parts of the meniscus when performing surgery to stabilize the knee. To address stifle instability many surgical treatment options are available. These different techniques can be lumped into two groups based on different concepts:
Osteotomy techniques
Osteotomy techniques require a bone cut (osteotomy) which changes the way the quadriceps muscles act on the top of the shin bone (tibial plateau). Stability of the stifle joint is achieved without replacing the CCL itself but rather by changing the biomechanics of the knee joint. This can be accomplished by either advancing the attachment of the muscle (tibial tuberosity advancement or TTA) or by rotation the plateau (slope) of the shin bone (tibial plateau leveling osteotomy or TPLO). Many surgeons prefer these techniques for large, active dogs, and at CSU we generally prefer the TPLO technique.

Tibial Plateau Leveling Osteotomy (TPLO)
Tibial plateau leveling osteotomy (TPLO) involves making a circular cut in the tibial plateau and rotating the contact surface of this bone until it attains a relatively level orientation that puts it at approximately 90 degrees to the attachment of the quadriceps muscles (see Figure 2). This orientation of the tibial plateau renders the knee relatively stable, independent of the CCL. The cut in the bone needs to be stabilized by the use of a bridging bone plate and screws. Once the bone has healed, the bone plate and screws are not needed, but are seldom removed unless there is an associated problem. The greatest advantage of this technique is the perceived superior outcome (limb function and less progression of arthritis) compared to traditional suture techniques especially in young, large breed dogs. The major disadvantage is the need to perform an osteotomy. Any osteotomy requires healing of the bone and if a problem is observed (such as implant failure, failure of the bone to heal), it may require multiple revision surgeries and the outcome may be poor. Luckily, such complications are rare, especially when the procedure is performed by an experienced surgeon.
Tibial Tuberosity Advancement (TTA)

Tibial tuberosity advancement (TTA) requires a linear cut along the front of the shin bone. The front of the tibia, called the “tibial tuberosity” is advanced forward until the attachment of the quadriceps is oriented approximately 90 degrees to the tibial plateau (notice that this is simply another way to accomplish the same orientation as the TPLO). Again, this orientation renders the knee stable, independent of the CCL. Similar to the TPLO, the cut in the bone is stabilized by the use of a specifically designed bridging bone plate and screws. The decision between TPLO and TTA is based upon concurrent problems, surgeon preference, etc. The anatomic configuration of some dog’s knees does not lend them to safe or effective application of this technique.
Suture techniques
Suture techniques can be divided into intra-articular (within the joint) and extra-articular (outside the joint) procedures. In humans intra-articular replacement of the ACL using some form of ACL replacement is the most common procedure. This approach has been studied extensively in dogs and found not to be successful mainly because of the difference in anatomy and underlying disease process. However, many companies and surgeons are revisiting this possibility utilizing novel developments. Because of the disappointment with intra-articular techniques to date, suture techniques are currently performed in an extra-articular fashion in dogs. The most commonly performed technique is called extra-capsular suture stabilization and utilizes strong suture material that is placed just on the outside of the knee joint (but under the skin) to mimic the CCL and stabilize the joint.
Extra-Capsular Suture Stabilization
Extra-capsular suture stabilization (also called “ex-cap suture,” “lateral fabellar suture stabilization,” and the “fishing line technique”) has been performed for many years. While there are many variations of this technique (different suture materials, ways to tie the suture, how to attach the suture to the bone, etc.), the general concept of this procedure is to replace the function of a defective CCL on the outside of the joint. This is usually accomplished by utilizing a strong suture placed along a similar orientation to the original cruciate ligament. The suture needs to stabilize the knee joint, while allowing normal knee movement, until organized scar tissue can form and assume the stabilizing role. The most common complications after this procedure involve failure of the suture and progressive development of arthritis. Suture failure tends to be more common in larger, active dogs; hence many surgeons reserve this technique for small breeds, older and/or inactive dogs. The main advantages of this technique include the lower cost and the lack of a bone cut (meaning that complications associated with the bone cut are not seen with this technique).
Potential Complications Following Surgical Treatment
When choosing the best treatment for your dog, possible complications should be considered. Complications that can be observed with any technique include complications associated with the anesthesia, wound problems, infection, patellar (knee cap) luxation (dislocation) and failure to return to normal function and progressive arthritis. Complications specific to the osteotomy techniques include delayed healing of the bone, non-healing of the bone, healing in an incorrect position (i.e. with rotation of the limb), fracture of the bone, and failure/breaking of the screws/plates. These complications can be serious and may require multiple revision surgeries. Again, serious complications that require a second surgery are rare when the procedures are performed by an experienced surgeon and exercise-restriction guidelines are followed.
Aftercare
Postoperative care at home is very critical. Premature, uncontrolled, or excessive activity risks complete or partial failure of the surgical repair. When choosing a suture repair, this failure may simply mean that the surgery has to be performed again, but when choosing an osteotomy technique this failure may mean that a much more invasive approach is now needed (application of an external fixator, for example). Proper postoperative care limits activity to leash walking for a minimum of eight weeks and no running, jumping, rough-housing, or off-leash activity. While it is important to control activity it is also important to maintain muscle mass and joint function (range of motion). Multiple studies have shown that physical therapy speeds the recovery and improves final outcome regardless of the chosen surgical technique. This rehabilitation should start immediately after surgery and usually includes a regime of passive range of motion, balance exercises, controlled walks on leash, etc. Please feel free to contact us to find out more about our post-operative rehabilitation protocols.
Prognosis
Long term prognosis for animals undergoing surgical repair of CCLD is good, with clinical reports of improvement in 85-90% of the cases. Unfortunately, arthritis progresses regardless of treatment, however much slower when surgery is performed. Therefore, medical arthritis management/prevention is recommended for any dog with CCLD regardless of the chosen surgical technique. It is important to realize that arthritis is a progressive disease and develops fairly quickly in an injured (or damaged) stifle joint. Hence, early surgical repair is advised by most surgeons. At CSU, we prefer to treat dogs with partial tears with surgery because this will decrease the amount of arthritis that has developed and decrease the chance of a meniscal tear to be found at surgery.
Treatment Options: Non-Surgical Treatment
Non-surgical treatment usually involves a combination of medications, exercise modification, joint supplements and possibly braces/orthotics.
Activity restriction and anti-inflammatories
The lameness associated with CCLD usually waxes and wanes and generally improves significantly with administration of pain medications (please note that dogs should not be given Aspirin). Especially in small dogs and with partial tears the lameness may completely disappear with this treatment but usually some degree of lameness remains in larger dogs. Attempts to return to normal activity levels will often be limited by the progression of arthritis. The combination of pain medications and rest is not a treatment per se because it does not stabilize the knee. Therefore, this treatment is generally not advised, but it may be appropriate for individual dogs due to some combination of their very small size, inactive lifestyle, other concurrent injuries or diseases, or financial realities.
Rehabilitation therapy

There is ample evidence that rehabilitation therapy by a trained rehabilitation practitioner can advance and hasten the recovery from surgery. However, there is little evidence to suggest that this is a consistent and predictable alternative to surgical management for most dogs. Occasionally the combination of concurrent injuries or diseases, advanced age, patient size, and financial limitations may make this an attractive alternative option.
Custom knee bracing/orthotics
Custom knee bracing is relatively new to canine orthopedics and hence there is little scientific evidence available. This treatment is valuable for the selected patient and we have treated many dogs at CSU with this option. Bracing is a temporary solution and therefore not ideal for young, active animals.
Prevention
As mentioned previously obesity and poor physical condition are risk factors for the development of CCLD. If your dog is overweight, a weight loss program might be advisable. Regular, daily activity is another important component of CCLD prevention. Joint supplements may also be given, but there is no data to show that it prevents CCLD.