Horner’s syndrome in dogs is a non-painful condition where the flight-fight innervation to the eye (sympathetic innervation) is interrupted. The condition usually occurs suddenly. The most common clinical signs of Horner’s syndrome are:
- Drooping of the eyelids on the affected side (ptosis)
- The pupil of the affected eye will be constricted/small (miosis)
- The affected eye often appears sunken (enophthalmos)
- The third eyelid of the affected eye may appear red and raised
The sympathetic innervation to the eye is rather long (coursing from brain, down the spinal cord, through the chest, past the ear and back up to the eye). Damage occurring anywhere along that path can result in Horner’s syndrome.
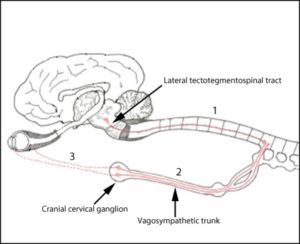
Horner’s syndrome is categorized into two phases: pre-ganglionic and post-ganglionic. We can attempt to differentiate between the two categories based on how (and how quickly) the eye responds to a drug that mimics sympathetic stimulation. Pre-ganglionic involvement (path 1 & 2 on the diagram) can be caused by infection, inflammation, injury, masses amongst other diseases and prognosis is usually more guarded. Post-ganglionic Horner’s syndrome means the affected area is closer to the eye (path 3 on the diagram). Middle or inner ear disease (otitis media or interna) can cause post-ganglionic Horner’s syndrome.
However, Horner’s syndrome in dogs is often classified as “idiopathic,” which means it is without known cause. This usually carries a much better prognosis. Any dog can develop Horner’s syndrome, although golden retrievers have a somewhat higher incidence. Most cases of Horner’s syndrome will resolve spontaneously, however for some dogs, the change will be permanent. It is important to treat any underlying disease. There are several diagnostic tests (baseline bloodwork, 4DX, otoscopic (ear) examination, 3 view thoracic radiographs including neck region) recommended to be performed to determine if there is an underlying cause in your pet.